Clinical Application of Functional Profiling
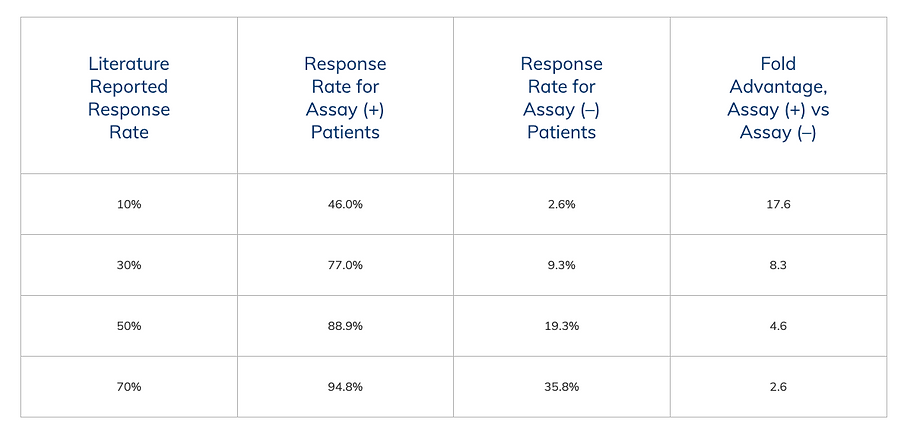
The following table is a representation of predicted clinical outcomes for patients treated with agents found active in the laboratory using the EVA-PCD functional profile.
With performance characteristics borrowed from the studies described earlier, these analyses have a sensitivity of 78.4% and specificity of 90.1%.
Literature Reported Response Rate
This column provides the expected clinical response rate based on current literature reported response rates (pre-test expectation).
These range from a 10% expected response rate for malignancies such as melanoma or renal cell carcinoma, up to 70% expected response rate for diseases such as untreated ovarian cancer or breast cancer.

Most Effective and Least Toxic Treatment
Currently, hundreds of drugs, drug combinations and targeted agents are used to treat cancer patients.
With so many choices, how does your oncologist decide which ones are right for you?
Generally, oncologists use established regimens developed through randomized clinical trials to prescribe chemotherapeutic agents. These regimens are average solutions for the “average” patient.
Regrettably, average treatments provide average outcomes, with the majority of patients failing to show significant improvement from these protocols.
Cancer is Unique
Each cancer patient is unique and their response to therapy is very different from one person to the next. Drugs that work for one patient may not work for another, even if they carry exactly the same diagnosis.
One way to help identify the best treatment option for you is to submit a living sample of your cancer cells for what we call a "functional profile".
Functional Profiling With Our EVA-PCD Assay
Functional profiling, is very different from genomic testing which is offered by most medical centers. Genomic testing looks for mutations and other changes in each patient's gene makeup that might guide drug selection. Although the concept is appealing, in reality, a minority of patients have genetic changes that can be used for therapy.
Functional profiling is a laboratory technique pioneered by Dr. Robert Nagourney, founder of Nagourney Cancer Institute, that measures how cancer cells respond when they are exposed to drugs and drug combinations.
We call it the Ex-Vivo Analysis of Programmed Cell Death (EVA-PCD) assay.
Programmed Cell Death is the Key
Put simply, it is a real-time measure of which drugs cause your cancer cells to die, through a process called programmed cell death.
By using this approach, we can determine in the laboratory the best drugs for each patient before they receive them.
The selection of drugs/agents used for testing are disease-specific and based on your diagnosis and previous treatment history.
We can customize the drugs tested based on your oncologist’s request.
A standard panel consists of 8 – 16 drugs/combinations.
Advances in Cancer Testing & Understanding Cancer Biology
Modern advances in our understanding of cancer biology have shown that cancer cells do NOT grow faster than normal cells, but instead, fail to die.
Cancers arise from cells that have learned certain tricks to enhance their survival so they can outlive their normal counterparts.
These transformed (cancerous) cells interact directly with their micro-environment. Cancer cells "talk" to each other and to all the surrounding cells using chemical signals like growth factors and byproducts of metabolism. Blood vessels, immune cells and connective tissues (stroma) all participate and contribute to the cancer process.
This is why it is absolutely essential to test cancers in their own natural clusters known as "microspheroids". We isolate these 3-dimensional structures directly from each patient's tumor to test drugs and combinations.
It is because we capture cancer in its native state that our approach is a very accurate platform for response prediction.
By using therapies found active in the laboratory through functional profiling, we have been able to double response rates and improve survival for patients.


